3月week3文献阅读:Dynamics of breast-cancer relapse reveal late-recurring ER-positive genomic subgroup
乳腺癌复发动态显示晚期复发的ER-阳性基因组亚群
摘要:
The rates and routes of lethal systemic spread in breast cancer are poorly understood owing to a lack of molecularly characterized patient cohorts with long-term, detailed follow-up data.
由于缺乏具有分子特征的患者群体和长期详细的随访数据,对乳腺癌致命全身扩散的发生率和途径知之甚少。
Longterm follow-up is especially important for those with oestrogenreceptor (ER)-positive breast cancers, which can recur up to two decades after initial diagnosis.
对于雌激素受体(ER)阳性的乳腺癌患者来说,长期随访尤为重要。乳腺癌在最初诊断后20年内可能复发。
It is therefore essential to identify patients who have a high risk of late relapse.
因此,确定晚期复发风险高的患者是至关重要的。
Here we present a statistical framework that models distinct disease stages (locoregional recurrence, distant recurrence, breast-cancer-related death and death from other causes) and competing risks of mortality from breast cancer, while yielding individual risk-of-recurrence predictions.
在此,我们提出了一个统计框架,该框架模拟了不同的疾病阶段(局部复发、远处复发、乳腺癌相关死亡和其他原因的死亡)和乳腺癌死亡率的竞争风险,同时给出了个体复发风险的预测。
We apply this model to 3,240 patients with breast cancer, including 1,980 for whom molecular data are available, and delineate spatiotemporal patterns of relapse across different categories of molecular information (namely immunohistochemical subtypes;PAM50 subtypes, which are based on gene-expression patterns;and integrative or IntClust subtypes, which are based on patterns of genomic copy-number alterations and gene expression12,13).
我们将该模型应用于3240例乳腺癌患者,其中1980例患者的分子数据可用,并描绘时间上不同类别的分子信息(即免疫组化亚型;PAM50亚型,基于基因表达模式;以及基于基因组拷贝数改变和基因表达模式的整合型或整合型(12,13)。
We identify four late-recurring integrative subtypes, comprising about one quarter (26%) of tumours that are both positive for ER and negative for human epidermal growth factor receptor 2, each with characteristic tumour-driving alterations in genomic copy number and a high risk of recurrence (mean 47–62%) up to 20 years after diagnosis.
我们识别四个late-recurring综合子类型,包括约四分之一(26%)的肿瘤,ER阳性和阴性人类表皮生长因子受体2,每个特征tumour-driving改变基因组拷贝数和高复发风险的(意思是47 - 62%)后20年的诊断。
We also define a subgroup of triplenegative breast cancers in which cancer rarely recurs after five years, and a separate subgroup in which patients remain at risk.
我们还定义了一个五年后癌症很少复发的三叉神经性乳腺癌的亚组,以及一个患者仍然处于危险中的单独的亚组。
Use of the integrative subtypes improves the prediction of late, distant relapse beyond what is possible with clinical covariates (nodal status, tumour size, tumour grade and immunohistochemical subtype).
综合亚型的使用提高了对晚期、远处复发的预测,超出了临床协变量(淋巴结状态、肿瘤大小、肿瘤分级和免疫组化亚型)的预测能力。
These findings highlight opportunities for improved patient stratification and biomarker-driven clinical trials.
这些发现强调了改善患者分层和生物标志物驱动临床试验的机会。
正文:
第一段
Breast cancer is a multistate disease with clinically relevant intermediate end points, such as locoregional recurrence and distant recurrence.
乳腺癌是一种多状态的疾病,具有临床相关的中间终点,如局部复发和远处复发。
A patient’s prognosis can differ considerably depending on when and where a relapse occurs, time since surgery, and time since locoregional or distant recurrence.
患者的预后可能因复发的时间和地点、手术后的时间以及局部或远处复发的时间而有很大差异。
These events are associated, and individual analyses of disease-free survival (DFS) or overall survival alone cannot fully capture patterns of recurrence associated with differential prognosis.
这些事件是相关的,单独对无病生存(DFS)或总体生存的个体分析不能完全捕获与不同预后相关的复发模式。
In addition, most survival analyses use disease-specific death (DSD) as the primary end point, and censor deaths from other causes.
此外,大多数生存分析使用疾病特异性死亡(DSD)作为主要终点,并审查来自其他原因的死亡。
However, when competing risks of mortality occur, this approach induces bias.
然而,当死亡率的竞争风险发生时,这种方法会导致偏见。
This is particularly problematic for breast cancer, where ER-positive patients experience higher mortality from nonmalignant causes owing to their increased age at diagnosis relative to ER-negative patients.
这对乳腺癌尤其成问题,在乳腺癌中,ER-阳性患者由于相对于ER-r阴性患者诊断年龄的增加,非恶性原因导致的死亡率更高。
乳腺癌预后现状以及乳腺癌生存分析存在问题。
第二段
We evaluated the extent of such bias on breast-cancer survival estimates by analysing 3,240 patients who had been diagnosed between 1977 and 2005, and for whom there was a median clinical follow-up of 14 years (referred to as the ‘full dataset’;see Extended Data Fig. 1, Supplementary Table 1 and Methods).
我们通过分析1977年至2005年间被诊断出乳腺癌的3240名患者评估了这种对乳腺癌生存评估的偏见程度,并对他们进行了14年的临床随访(称为“完整数据集”;参见扩展数据图1、补充表1和方法)。
We compared the naive cumulative incidence for DSD (computed as one minus the survival probability), stratified by ER status and considering only cancer-related deaths (Extended Data Fig. 2a), relative to estimates with the proper cumulative incidence functions accounting for different causes of death (Extended Data Fig. 2b).
我们比较了单纯的DSD累积发病率(计算为1减去生存概率),按ER状态分层,只考虑与癌症相关的死亡(扩展数据图2a),相对于使用适当的累积发病率函数估计不同的死亡原因(扩展数据图2b)。
These comparisons indicate that the incidence of DSD is overestimated for ER-positive tumours relative to ER-negative tumours (0.46 versus 0.37 at 20 years) owing to the increased age of diagnosis (median 63.9 versus 53.0 years;P < 1 × 10−6;Extended Data Fig. 2c).
这些比较表明,由于诊断年龄的增加(中位数63.9岁对53.0岁), ER-阳性肿瘤相对于 ER-阴性肿瘤的DSD发生率被高估(20岁时为0.46对0.37);P < 1×10 - 6;扩展数据图2c)。
Moreover, because the baseline survival functions for these subgroups are distinct, their differences cannot be adequately summarized with a single parameter in a Cox proportional hazards model.
此外,由于这些亚组的基线生存函数是不同的,因此不能用Cox比例危险模型中的单个参数充分总结它们之间的差异。
(构建数据分析数据集,证实生存分析使用疾病特异性死亡(DSD)的偏见程度,探索ER和DSD复发的关系,结论:诊断年龄的增加(中位数63.9岁对53.0岁), ER-阳性肿瘤相对于 ER-阴性肿瘤的DSD发生率被高估(20岁时为0.46对0.37);P < 1×10 - 6;扩展数据图2c。数据+图,总结分析结果)
第三段
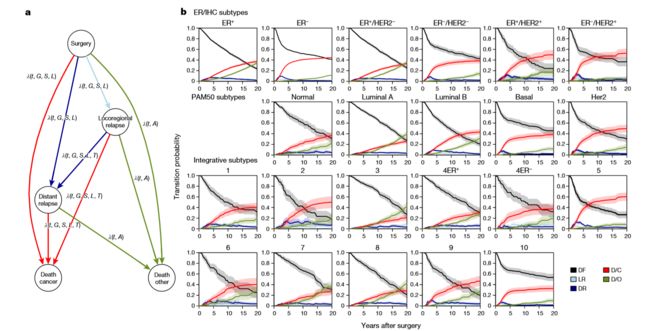
To overcome these limitations, we developed a nonhomogenous (semi)-Markov-chain model that accounts for different disease states (locoregional recurrence and distant recurrence) and time scales (time since surgery or locoregional or distant recurrence), as well as competing risks of mortality and distinct baseline hazards across molecular subgroups, thereby enabling individual risk-of-relapse predictions (see Fig. 1a and Methods).
为了克服这些限制,我们开发了一个针对非(半)马尔可夫链模型,占不同疾病状态(局部区域复发和远处复发)和时间尺度(时间因为手术或局部区域或遥远的复发),以及竞争风险的死亡率和不同的基线危险分子子组,从而使个人risk-of-relapse预测和方法(见图1)。
The model also incorporates clinical variables known to influence breast-cancer survival,including age, tumour grade, tumour size and number of tumour-positive (‘positive’) lymph nodes (all measured at diagnosis).
该模型还纳入了已知影响乳腺癌生存的临床变量,包括年龄、肿瘤分级、肿瘤大小和肿瘤阳性(“阳性”)淋巴结数量(所有在诊断时测量的)。
We refer to this as the base clinical model, into which information on molecular subtype can be incorporated.
我们将其作为基本的临床模型,将分子亚型的信息纳入其中。
(作者研究开发的模型,克服当下模型的局限。)
第四段
We fitted this multistate model to the full dataset, and recorded the hazards of moving through distinct states and the number of transitions between each pair of states (Supplementary Table 2 and Methods).
我们将这个多状态模型拟合到完整的数据集中,并记录了通过不同状态移动的风险以及每对状态之间的转换次数(补充表2和方法)。
As expected, most cancer-related deaths (83% in ER-positive and 87% in ER-negative tumours) occurred after distant metastasis.
不出所料,大多数与癌症相关的死亡(83%的er阳性肿瘤和87%的er阴性肿瘤)发生在远处转移之后。
The remainder of the cases probably reflect undetected recurrences or death due to other malignancies.
其余病例可能反映未发现的复发或因其他恶性肿瘤死亡。
Age at diagnosis was associated with a transition to death by other causes (P < 1 × 10−6).
诊断年龄与其他原因引起的死亡过渡有关(P < 1×10 - 6)。
Examination of the log hazard ratios and 95% confidence intervals for all other variables indicated that their effect decreased with disease progression (Extended Data Fig. 2d).
对所有其他变量的log危险比和95%置信区间的检查表明,它们的影响随着疾病进展而降低(扩展数据图2d)。
That is, clinical variables related to the primary tumour were more prognostic for earlier transitions than for later transitions.
也就是说,与原发肿瘤相关的临床变量对早期转移的预后比晚期转移的预后更好。
However, several tumour characteristics informed the risk of progression from locoregional to distant recurrence, and from distant recurrence to death.
然而,一些肿瘤特征提示了从局部到远处复发以及从远处复发到死亡的风险。
In ER-positive disease, higher tumour grade, number of positive lymph nodes and tumour size all increased the risk of progression to a later state.
在er阳性的疾病中,较高的肿瘤分级、阳性淋巴结数目和肿瘤大小都增加了进展到晚期的风险。
A longer time between surgery and locoregional or distant recurrence decreased the risk of transition to a later state, and was more pronounced in ER-negative disease.
手术和局部或远处复发之间的较长时间降低了向晚期转移的风险,在er阴性疾病中更明显。
(作者们提出的模型分析数据证实,图和文献双证实。)
第五段
A notable feature of our multistate model is that hazard rates can be transformed into transition probabilities that represent the probability of moving from one state into another after a given time.
我们的多状态模型的一个显著特征是,危险率可以转换为表示在给定时间后从一个状态转移到另一个状态的概率的转移概率。
To evaluate patterns of recurrence across established breast-cancer molecular subgroups, we turned to the Molecular Taxonomy of Breast Cancer International Consortium (METABRIC) molecular dataset.
为了评估乳腺癌分子亚群的复发模式,我们求助于乳腺癌国际联盟(METABRIC)分子数据集的分子分类学。
This dataset is based on 1,980 patients (Extended Data Fig. 1), and includes assignments to: immunohistochemistry (IHC) subtypes (namely ER+/ HER2+, ER+/HER2−, ER−/HER2+ and ER−/HER2−, where HER2 is human epidermal growth factor receptor 2);5 intrinsic gene-expression subtypes (otherwise known as PAM50 subtypes);and the 11 Integrative Cluster (IntClust) subtypes, which are characterized by distinct copy-number and gene-expression profiles (Supplementary Table 3). We computed the baseline transition probabilities from surgery, locoregional recurrence or distant recurrence at various time intervals (2, 5, 10, 15 and 20 years) and the corresponding standard errors of prediction (s.e.) for average individuals in each subgroup (using the full dataset for comparisons by ER status,and the molecular dataset for all others;Supplementary Table 4).
该数据集基于1980名患者(扩展数据图1),包括分配给:免疫组化(IHC)亚型(即ER+/HER2 +、ER+/HER2−、ER−/HER2+和ER−/HER2−,其中HER2是人类表皮生长因子受体2);5个内在基因表达亚型(又称PAM50亚型)和11综合集群(IntClust)亚型,特点是独特的人类基因组和基因表达profiles(补充表3)。我们从手术基线转移概率计算,局部区域复发或远处复发在不同的时间间隔(2、5、10、15、20年)和相应的标准误差的预测(东南部)的平均个人每个子群(使用ER状态的完整数据集的比较,以及其他所有的分子数据集;补充表4)。
(分子数据集分类,采用乳腺癌国际联盟分子数据集的分子分类)
第六段
After surgery, state transitions differed substantially across the various subtypes (Fig. 1b).
手术后,不同亚型的状态转变有很大差异(图1b)。
For example, the transition probabilities post-surgery reveal different change points for ER-positive versus ER-negative disease.
例如,术后转移概率显示er阳性和er阴性疾病的不同变化点。
ER-negative patients had a higher risk of distant recurrence and death from cancer in the first five years, after which their risk decreased considerably.
er阴性的患者在前五年有更高的癌症复发和死亡的风险,之后他们的风险大大降低。
By contrast, ER-positive patients had a smaller but longer risk period during the first ten years, and the risk increased at a lower rate.
相比之下,er阳性患者在前十年的风险期较小,但较长,并且风险以较低的速度增加。
Among ER-negative patients, the PAM50 ‘basal-like’ subgroup was nearly indistinguishable from the ER−/HER2− subgroup, with most cancer-related deaths occurring in the first five years—similar to HER2+ patients (before the widespread use of trastuzumab).
在ER阴性患者中,PAM50“碱性”亚组与ER- /HER2 -亚组几乎没有区别,大多数癌症相关死亡发生在前5年,与HER2+患者相似(在曲妥珠单抗广泛使用之前)。
By contrast, the three predominantly ER-negative IntClust subgroups (IntClust4ER−, IntClust5 and IntClust10) exhibited substantial differences in their recurrence trajectories.
相比之下,三个主要为er阴性的IntClust亚群(IntClust4ER−、IntClust5和IntClust10)的复发轨迹有显著差异。
As expected, IntClust5 (HER2+ enriched) generally had poor prognosis at 5 years (transition probability to relapse/cancer-related death 0.48;s.e = 0.04), with the risk increasing to 0.65 (s.e. = 0.04) at 20 years.
正如所料,IntClust5 (HER2+富集)一般在5年时预后较差(复发/癌症相关死亡的转移概率为0.48;s.e = 0.04), 20年后风险增加到0.65 (s.e. = 0.04)。
For IntClust10 (‘basal-like enriched’), the first 5 years after surgery largely defined patient outcomes: the probability of relapse or cancer-related death at 5 years was 0.33 (s.e. = 0.03), and this rose after 20 years only to 0.37 (s.e. = 0.04) for an average patient.
对于IntClust10(“基底样富集”),手术后的前5年在很大程度上定义了患者的预后:5岁时复发或癌症相关死亡的概率为0.33 (s.e. = 0.03),而20年后这一数字仅上升到平均患者的0.37 (s.e. = 0.04)。
This pattern was distinct from that seen for IntClust4ER− patients, who exhibited a persistent and increasing risk of relapse or cancer-related death with a probability of 0.30 (0.05) at 5 years and 0.49 (0.05) after 20 years.
这一模式与IntClust4ER -患者不同,后者在5年后复发或癌症相关死亡的风险为0.30(0.05),在20年后为0.49(0.05),并且持续增加。
(数据集分类分析后的亚型的状态转变差异例举说明)
第七段
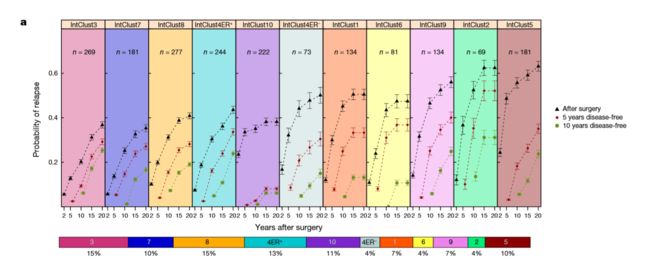
The distinction between IntClust4ER− and IntClust10 is also apparent when examining the average probabilities of relapse among all patients across the IntClust subtypes after surgery or after being disease-free for five and ten years (Fig. 2a).
IntClust4ER -和IntClust10之间的区别在检查所有IntClust亚型患者术后或无病5年和10年后复发的平均概率时也很明显(图2a)。
Indeed, through the course of the disease, the risk of relapse changed considerably across the integrative subtypes, and to a lesser extent across the IHC and PAM50 subtypes (Fig. 2a and Extended Data Fig. 4). Moreover, the probabilities of distant recurrence or cancer-related death among ER−/HER2− patients who were disease-free at five years after diagnosis revealed low (IntClust10) and high (IntClust4ER−) risks for late-relapse triple-negative breast-cancer (TNBC) subgroups,whereas IHC (and PAM50) subtypes homogenized this risk (Extended Data Fig. 5).
事实上,病程,复发的风险大大改变了整个综合亚型,和一定程度上在IHC和PAM50亚型(图2和扩展数据图。4)。此外,远处复发的概率或癌症相关死亡中ER / HER2−−患者在诊断后5年无病显示低(IntClust10)、高(IntClust4ER−)风险诱发late-relapse三阴乳腺癌(TNBC)子组,而IHC(和PAM50)亚型均有这种风险(扩展数据见图5)。
(进一步解释数据集分析结果)
第八段
Marked differences were also apparent among ER-positive patients, with patients with IntClust3, IntClust7, IntClust8 and IntClust4ER+ subtypes exhibiting a better prognosis, whereas patients with IntClust1, IntClust2, IntClust6 and IntClust9 subtypes exibited late-recurring cancer with a poor prognosis (Fig. 2a).
er阳性患者之间也存在显著差异,其中IntClust3、IntClust7、IntClust8、IntClust4ER+亚型预后较好,而IntClust1、IntClust2、IntClust6、IntClust9亚型患者存在晚期复发性肿瘤,预后较差(图2a)。
These latter four subgroups had an exceedingly high risk of relapse, with mean probabilities ranging from 0.47 to 0.62 up to 20 years after surgery.
后四个亚组的复发风险非常高,术后20年的平均复发概率在0.47到0.62之间。
The IntClust2 subtype exhibited the worst prognosis, with a probability of relapse (0.62;s.e.m. = 0.02) second only to that of IntClust5.
IntClust2亚型预后最差,有复发的可能性(0.62;s.e.m. = 0.02)仅次于IntClust5。
Collectively, these subgroups comprise 26% of ER-positive cases (Fig. 2b, c) and thus define the minority of patients who may benefit from extended monitoring and treatment given the chronic nature of their disease.
总的来说,这些亚组构成了26%的er阳性病例(图2b, c),从而确定了少数患者可能受益于延长监测和治疗鉴于他们的疾病的慢性性质。
(不同亚型的预后说明)
第九段
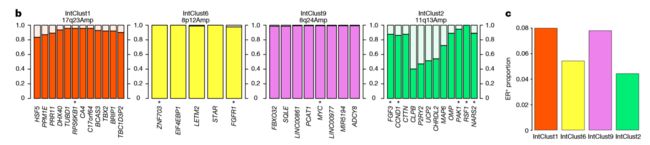
Importantly, the four ‘high risk of relapse’ subgroups were enriched in characteristic genomic-copy-number alterations, which represent the likely drivers of each subgroup (Fig. 2b).
重要的是,四个“高复发风险”亚组在特征基因组拷贝数改变上得到了丰富,这代表了每个亚组的可能驱动因素(图2b)。
For example, IntClust2 tumours are defined by amplification and concomitant overexpression of multiple oncogenes on chromosome 11q13, including CCND1, FGF3, EMSY, PAK1 and RSF1 (refs 20–22).
例如,IntClust2肿瘤定义为11q13号染色体上多个癌基因的扩增和伴随过表达,包括CCND1、FGF3、EMSY、PAK1和RSF1(参考文献20-22)。
IntClust2 accounts for 4.5% of ER-positive cases, 96% of which have RSF1 amplification, compared with 0–22% in other subgroups.
在er阳性病例中,IntClust2占4.5%,其中96%具有RSF1扩增,而在其他亚组中,这一比例为0-22%。
IntClust6 (5.5% of ER-positive tumours) is characterized by focal amplification of ZNF703 (ref. 23) and FGFR1 (ref. 24) on chromosome 8p12 (100% of IntClust6 cases versus 2–21% of others).
IntClust6(5.5%的er阳性肿瘤)的特征是ZNF703(参考文献23)和FGFR1(参考文献24)在8p12染色体上的局灶性扩增(100%的IntClust6病例和2-21%的其他病例)。
IntClust1 (8% of ER-positive tumours) exhibited amplification of chromosome 17q23 in a region spanning the mTOR effector RPS6KB1 (also known as S6K1)25, which was gained or amplified in 96% and 70% of cases, respectively (versus amplification in 0–25% of other subtypes).
IntClust1(8%的er阳性肿瘤)在横跨mTOR效应子RPS6KB1(也称为S6K1)25的区域表现出17q23染色体的扩增,96%和70%的病例分别获得或扩增了该区域(而其他亚型的扩增率为0-25%)。
IntClust9 accounted for another 8% of ER-positive cases and was characterized by amplification of the MYC oncogene at chromosome 8q24, with amplification in 89% of these tumours (versus 3–42% of other groups).
在er阳性病例中,IntClust9占8%,其特征是8q24号染色体上MYC癌基因的扩增,其中89%的肿瘤中存在扩增(其他组为3-42%)。
Thus the late-recurring ER-positive subgroups are defined by genomic drivers, several of which are viable therapeutic targets.
因此,晚期复发的er阳性亚群是由基因组驱动决定的,其中一些是可行的治疗靶点。
(图分析结果说明+文献论证)
第十段
Similar differences in the probability of late, distant relapse were seen in the subset of patients whose tumours were ER+/HER2− (Fig. 3a, b and Extended Data Fig. 4a–f)—a group in which late relapse and strategies to target this, such as extended endocrine therapy, represent critical clinical challenges.
在肿瘤为ER+/HER2−(图3a、b和扩展数据图4a-f)的患者亚群中,晚期复发和远处复发的概率存在类似的差异,其中晚期复发和针对这一目标的策略,如延长内分泌治疗,代表了关键的临床挑战。
In particular, the probabilities of distant recurrence or cancer-related death reveal a significant risk for IntClust subtypes 1, 2, 6 and 9 (relative to IntClust3) that varied over time.
特别是,与IntClust3相比,远端复发或癌症相关死亡的概率揭示了IntClust亚型1、2、6和9(相对于IntClust3)随时间变化的显著风险。
Moreover, the risk was not fully captured by a model that included IHC subtype together with clinical variables (age, tumour size, grade, number of positive lymph nodes and time since surgery) that have been shown to dictate distant-relapse outcomes even after a long disease-free interval5 (Fig. 3a).
此外,包括IHC亚型和临床变量(年龄、肿瘤大小、分级、阳性淋巴结数目和手术后时间)在内的模型并没有完全捕捉到这种风险,这些临床变量已经表明,即使在长时间无病间隔后,也会决定远处复发的结果(图3a)。

We therefore assessed whether the integrative subtypes provide information about a patient’s risk of late distant relapse above and beyond what could be inferred optimally from standard clinical information.
因此,我们评估了综合亚型是否提供了关于患者晚期远处复发风险的信息,这些信息超出了可以从标准临床信息中推断出的最佳水平。

We found that the model including clinical variables combined with IHC subtype provided substantial information about the probability of distant relapse in ER+/HER2− patients who were relapse free at five years.
我们发现,包括临床变量和IHC亚型的模型提供了关于ER+/HER2−患者5年无复发的远期复发概率的大量信息。
The concordance index (C-index) predicting the risk of distant relapse was 0.63 (confidence interval 0.58–0.68) at 10 years, 0.62 (0.58–0.67) at 15 years, and 0.61 (0.57–0.66) at 20 years (Fig. 3c).
预测远处复发风险的一致性指数(c指数)10年为0.63(置信区间0.58-0.68),15年为0.62(0.58-0.67),20年为0.61(0.57-0.66)(图3c)。
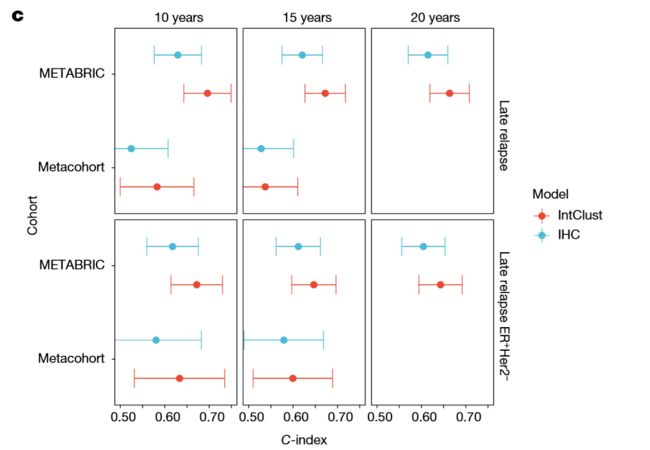
However, including the IntClust subtypes significantly improved the predictive value: the C-index was 0.70 (confidence interval 0.64–0.75;improvement over the clinical model, P = 0.00011) at 10 years, 0.67 (0.63–0.72;P = 0.0016) at 15 years and 0.66 (0.62–0.71;P = 0.0017) at 20 years.
然而,包括IntClust亚型的预测值显著提高:c指数为0.70(置信区间为0.64-0.75;相对于临床模型的改进,P = 0.00011) 10年后为0.67 (0.63-0.72;15年和0.66年(0.62-0.71;20年后P = 0.0017)。
These trends were recapitulated in an external validation cohort, despite the smaller sample size and shorter follow-up times (prohibiting analyses at 20 years) (Fig. 3c and Extended Data Fig. 3e).
尽管样本量更小,随访时间更短(禁止20年进行分析)(图3c和扩展数据图3e),但这些趋势在外部验证队列中得到了再现。
Thus, information about the dynamics of late relapse that is provided by integrative subtype could not be inferred from standard clinical variables, including IHC subtype.
因此,综合亚型提供的晚期复发动力学信息不能从包括IHC亚型在内的标准临床变量中推断出来。
(晚期复发和远处复发,综合亚型提供的复发动力学信息验证和局限)
第十一段
We next turned to the subset of patients who experienced a locoregional recurrence.
接下来我们转向经历局部复发的患者。
Such a relapse is commonly treated with curative intent, and is thought to be a high-risk event that is associated with increased rates (45–80%) of distant relapse28.
这种复发通常是有治疗目的的,被认为是一种高风险事件,与远处复发的发生率增加有关(45-80%)。
The transition probabilities after locoregional recurrence varied substantially depending on the pathological features of the primary tumour at diagnosis and the molecular subtype, highlighting opportunities for intervention (Extended Data Figs. 6, 7 and Supplementary Tables 2, 3). By contrast, after the initial distant relapse, all subgroups exhibited a high probability of cancer-related death, although the median times differed (Extended Data Fig. 8 and Supplementary Tables 2, 3).
局部区域复发后的跃迁概率差异很大取决于原发性肿瘤的病理特点在诊断和分子亚型,强调干预的机会(扩展数据无花果。6、7和补充表2、3)。相比之下,在最初的遥远的复发,所有子组表现出高概率的癌症相关的死亡,尽管中位数乘以不同(图8和扩展数据补充表2、3)。
(局部复发,综合亚型提供的动力学信息)
第十二段
Unique to our cohort is a subset of 618 patients (out of the 1,079 from the full dataset who relapsed) for whom a complete description of all recurrences is available (this is the recurrent-event dataset).
我们的队列中唯一的一个子集是618名患者(从完整的复发数据集中的1079名患者中选出),他们可以获得所有复发的完整描述(这是递归事件数据集)。
This enables a detailed analysis of the rates and routes of distant metastases and their lethality.
这使我们能够详细分析远处转移的速度和途径及其致命性。
These data reveal the varied time course over which metastases occurred and indicate that no sites of metastasis are exclusive to ER-positive or ER-negative disease (Extended Data Fig. 9a).
这些数据揭示了转移发生的不同时间进程,并表明没有转移位点是er阳性或er阴性疾病所独有的(扩展数据图9a)。
Moreover, multiple distant metastases were common, even among subgroups with a favourable prognosis (Extended Data Fig. 9b).
此外,即使在预后良好的亚组中,多发远处转移也是常见的(扩展数据图9b)。
We next examined the cumulative incidence and number of metastases at different organ sites stratified by ER status (Fig. 4a).
接下来,我们检查了按ER状态分层的不同器官部位的累积发病率和转移数(图4a)。
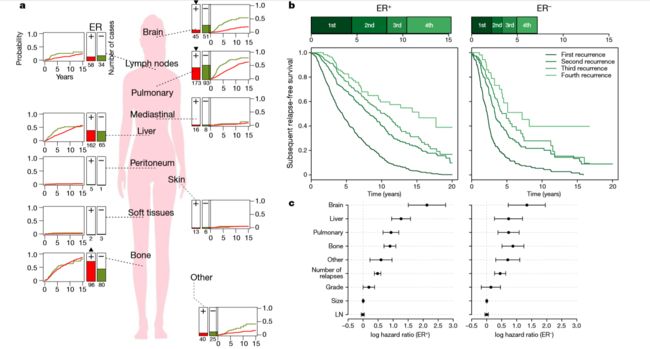
ER-negative cases harboured substantially more visceral disease than did ER-positive cases (for example, brain/meningeal, 27% versus 11%;pulmonary, 50% versus 41%).
er阴性病例比er阳性病例有更多的内脏疾病(例如,大脑/脑膜,27%对11%;肺部,50%对41%)。
As previously reported29,30, bone metastases were more common in ER-positive than in ER-negative cases (71% versus 43%), but the cumulative incidence was similar.
正如先前报道的29,30,骨转移在er阳性病例中比在er阴性病例中更常见(71%对43%),但累积发病率相似。
Thus, the higher proportions observed in ER-positive disease appear not to reflect site- specific tropism: rather, bone metastases take a long time to develop, and ER-negative patients tend to die of other metastases first.
因此,在er阳性疾病中观察到的较高比例似乎并不反映部位特异性取向:相反,骨转移需要很长时间才能发生,er阴性患者往往首先死于其他转移。
In addition, ER-positive tumours more commonly presented with a first metastasis in the bone (76% versus 61%).
此外,er阳性肿瘤更常见的表现为骨内首次转移(76%对61%)。
Similar comparisons stratified by IHC, PAM50 and IntClust subtypes reveal additional variability (Extended Data Fig. 10).
IHC、PAM50和IntClust亚型的类似比较揭示了额外的可变性(扩展数据图10)。
Striking differences in the rates of distant metastasis are also evident: ER-negative disease was characterized by a rapid series of relapses early after diagnosis, while most ER-positive patients suffered just one early relapse (commonly bone metastases), and if a second relapse occurred, the probability of additional relapses increased (Fig. 4b and Methods).
引人注目的远处转移率差异也很明显:er阴性疾病特点是一系列快速的复发早期诊断后,虽然大多数雌激素受体阳性患者有一个早期复发骨转移(通常),如果发生了第二次复发,额外的复发的概率增加(图4 b和方法)。
Thus, after distant recurrence, subtype continues to dictate the rate of subsequent metastases, underscoring the importance of tumour biology.
因此,在远处复发后,亚型继续决定随后转移的速度,强调肿瘤生物学的重要性。
Both the number and the site of relapses influenced the risk of death after recurrence, with brain metastasis being most predictive.
复发的数量和部位都影响复发后死亡的风险,其中脑转移是最具预测性的。
Risk estimates (Fig. 4c) were comparable between ER-positive and ER-negative tumours, suggesting that the impact of the site of metastasis on progression to death is similar.
er阳性和er阴性肿瘤的风险估计(图4c)相似,提示转移部位对死亡进展的影响相似。
(ER状态分层的不同器官部位的累积发病率和转移数,数据集的进一步分析解释,ER与肿瘤风险评估)
第十三段
In summary, by leveraging a cohort of 3,240 patients—including 1,980 from METABRIC, for whom detailed molecular characterization and recurrence data are available—we have delineated the spatiotemporal dynamics of breast-cancer relapse at a high resolution.
总之,通过利用3240名患者(包括1980名来自METABRIC的患者,他们有详细的分子特征和复发数据),我们以高分辨率描绘了乳腺癌复发的时空动态。
Our analyses are based on a multistate statistical model that yields individual risk-of-relapse estimates, using tumour features, clinical, pathological and molecular covariates, and disease chronology, and is available via a web application (https://caldaslab.cruk.cam.ac.uk/brcarepred).
我们的分析基于一个多状态统计模型,该模型利用肿瘤特征、临床、病理和分子共变量以及疾病年代学,得出个体复发风险的估计,并可通过web应用程序获得(https://caldaslab.cruk.cam.ac.uk/brcarepred)。
In contrast to existing models used to calculate the benefits of adjuvant therapy at diagnosis, such as PREDICT18, our research tool can be used to assess how a patient’s risk of recurrence changes throughout follow-up.
与用于计算诊断时辅助治疗的益处的现有模型(如PREDICT18)相比,我们的研究工具可用于评估患者在随访期间复发风险的变化。
Learning whether specific treatments change the outcomes of different integrative subtypes is important and will require analysis of randomized clinical trial cohorts.
了解特定治疗是否会改变不同综合亚型的结果是很重要的,这需要对随机临床试验进行分析。
(多状态统计模型总结,通过web应用程序获得(https://caldaslab.cruk.cam.ac.uk/brcarepred))。
第十四段
By classifying breast tumours into the 11 integrative subtypes, important differences in recurrence rates have become apparent that were obscured in the IHC and PAM50 subtypes.
通过将乳腺肿瘤分为11个综合亚型,复发率的重要差异变得很明显,而这在IHC和PAM50亚型中是不明显的。
Among TNBC patients, the IntClust10 cluster remains largely relapse free after five years, whereas IntClust4ER− patients continue to be at a substantial risk of recurrence.
在TNBC患者中,IntClust10组患者在5年后基本没有复发,而IntClust4ER -患者仍有很大的复发风险。
Among ER+/HER2− patients, IntClust subtypes 1, 2, 6 and 9 have a markedly increased risk of distant relapse up to 20 years after diagnosis, and together account for around one quarter of all ER-positive tumours and the vast majority of late recurrences.
在ER+/HER2−患者中,IntClust亚型1、2、6和9在诊断后20年远端复发的风险显著增加,它们加在一起约占所有ER阳性肿瘤的四分之一,且绝大多数晚期复发。
Moreover, the integrative subtypes markedly improved the prediction of distant recurrence after five years in ER+/HER2− patients.
此外,综合亚型显著提高了ER+/HER2−患者5年后远处复发的预测。
Our findings thus address one of the contemporary challenges in breast oncology, namely identification of the subset of ER-positive patients who have a high risk of recurrence and tumour biomarkers that are more predictive of recurrence than are standard clinical covariates7,8.
因此,我们的研究结果解决了乳腺肿瘤学当前面临的挑战之一,即确定er阳性患者中复发风险较高的子集,以及比标准临床协变量更能预测复发的肿瘤生物标志物。
Integrative subtyping may help to determine whether women who are relapse free five years after diagnosis might benefit from extended endocrine therapy or other interventions to improve late outcomes.
综合分型可能有助于确定诊断后5年无复发的妇女是否可能受益于延长内分泌治疗或其他干预措施,以改善晚期结果。
Critically, the four late-recurring ER-positive subgroups are enriched for genomic-copy-number driver alterations that can be therapeutically targeted, paving the way for new treatment strategies for these high-risk patient populations.
至关重要的是,这四个晚期复发的er阳性亚群的基因拷贝数驱动因子的改变,可作为治疗的目标,为这些高风险患者群体的新治疗策略铺平了道路。
(乳腺肿瘤分为11个综合亚型总结和意义)
Online content
在线内容:
Any methods, additional references, Nature Research reporting summaries, source data, statements of data availability and associated accession codes are available at https://doi.org/10.1038/s41586-019-1007-8.
任何方法、额外参考文献、自然研究报告摘要、源数据、数据可用性声明和相关的加入代码均可在https://doi.org/10.1038/s41586-019-1007-8获得。
医学信息挖掘:
后续研究点:(多状态统计模型研究)
提出了一个统计框架,该框架模拟了不同的疾病阶段(局部复发、远处复发、乳腺癌相关死亡和其他原因的死亡)和乳腺癌死亡率的竞争风险,同时给出了个体复发风险的预测
(多状态统计模型总结,通过web应用程序获得(https://caldaslab.cruk.cam.ac.uk/brcarepred))。